
GLP-1 Drugs and Metabolic Rate: What Happens to Your Metabolism?
GLP-1 medications change how much you eat — but do they change how your body burns energy? Here is what the research actually shows about metabolism, weight loss, and these widely-used drugs.
Millions of people are taking GLP-1 receptor agonist drugs like semaglutide and tirzepatide for weight loss. A common question is whether these drugs slow down metabolism — and whether that makes it harder to keep weight off long-term. This article explains what metabolic rate is, how GLP-1 drugs affect it, why muscle mass matters, and what you can do to support a healthy metabolism during and after treatment.
1. Introduction
GLP-1 receptor agonist drugs have become some of the most talked-about medications in the world. Drugs like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) help people lose 15–20% of their body weight over a year or more. For many people, this is life-changing.
But questions about what happens after — and underneath — that weight loss are growing louder. One of the most common is this: Do these drugs slow down your metabolism?
It is a fair question. Many people have heard that dieting slows metabolism. They worry that losing weight quickly on a powerful drug could make their metabolism permanently sluggish — or that stopping the drug could lead to rapid weight regain because their body has adjusted to burning fewer calories.
The answer is nuanced. GLP-1 drugs do not directly slow metabolism in the way that popular culture describes. But weight loss itself — regardless of how it happens — does lower the number of calories your body burns each day. And how much muscle you lose during that weight loss has a large effect on how much your metabolism slows.
This article unpacks all of that in plain language. No jargon, no oversimplification — just what the science actually says.
2. What Is Metabolic Rate?
Your metabolic rate is simply the speed at which your body uses energy. Every minute of every day — whether you are asleep, sitting at a desk, or running — your body is burning calories to keep you alive and functioning.
Total daily energy expenditure — the full amount of energy your body uses in a day — comes from three main sources:
The largest piece — basal metabolic rate, or BMR — is determined mostly by your body size and composition. A larger body needs more energy to run. More muscle tissue means a higher BMR, because muscle is metabolically active even at rest. More fat tissue means less, because fat cells burn far fewer calories than muscle cells.
This is why body composition — the ratio of muscle to fat in your body — matters so much for metabolism. It is not just about how much you weigh. It is about what that weight is made of.
Your metabolism is how fast your body burns calories. Most of it happens automatically, just keeping you alive. The biggest factors that control it are your body size and how much muscle you have. Lose weight — especially muscle — and your metabolism slows. Keep your muscle while losing fat, and your metabolism holds up much better.
3. How GLP-1 Drugs Work
To understand what GLP-1 drugs do to metabolism, you first need to understand what they actually do in the body.
GLP-1 stands for glucagon-like peptide-1. It is a hormone your gut naturally releases after you eat. It sends signals to your brain to reduce hunger, to your stomach to slow digestion, and to your pancreas to release insulin. The overall effect is that you feel full faster, stay full longer, and eat less.
GLP-1 receptor agonist drugs mimic and amplify this hormone. They bind to the same receptors that natural GLP-1 uses, but they stay active in the body much longer — days instead of minutes. The result is a sustained reduction in appetite and caloric intake.
Drug is injected or taken orally once weekly
GLP-1 receptor agonists like semaglutide are typically given as a once-weekly injection. Tirzepatide targets both GLP-1 and GIP receptors, making it a dual agonist with stronger effects at higher doses.
Brain receives reduced hunger signals
The drug activates GLP-1 receptors in the hypothalamus — the part of the brain that controls hunger and satiety. The result is a significant reduction in appetite and food cravings, often described by patients as "food noise" turning down dramatically.
Stomach empties more slowly
GLP-1 drugs slow gastric emptying — the speed at which food moves from your stomach into your small intestine. This extends the feeling of fullness after meals and reduces postmeal blood sugar spikes.
Caloric intake falls significantly
Because hunger is suppressed and fullness lasts longer, people eat substantially less. Studies show average caloric intake may fall by 25–35% during active GLP-1 treatment. This caloric deficit is the primary driver of weight loss — not any direct change to how the body burns energy.
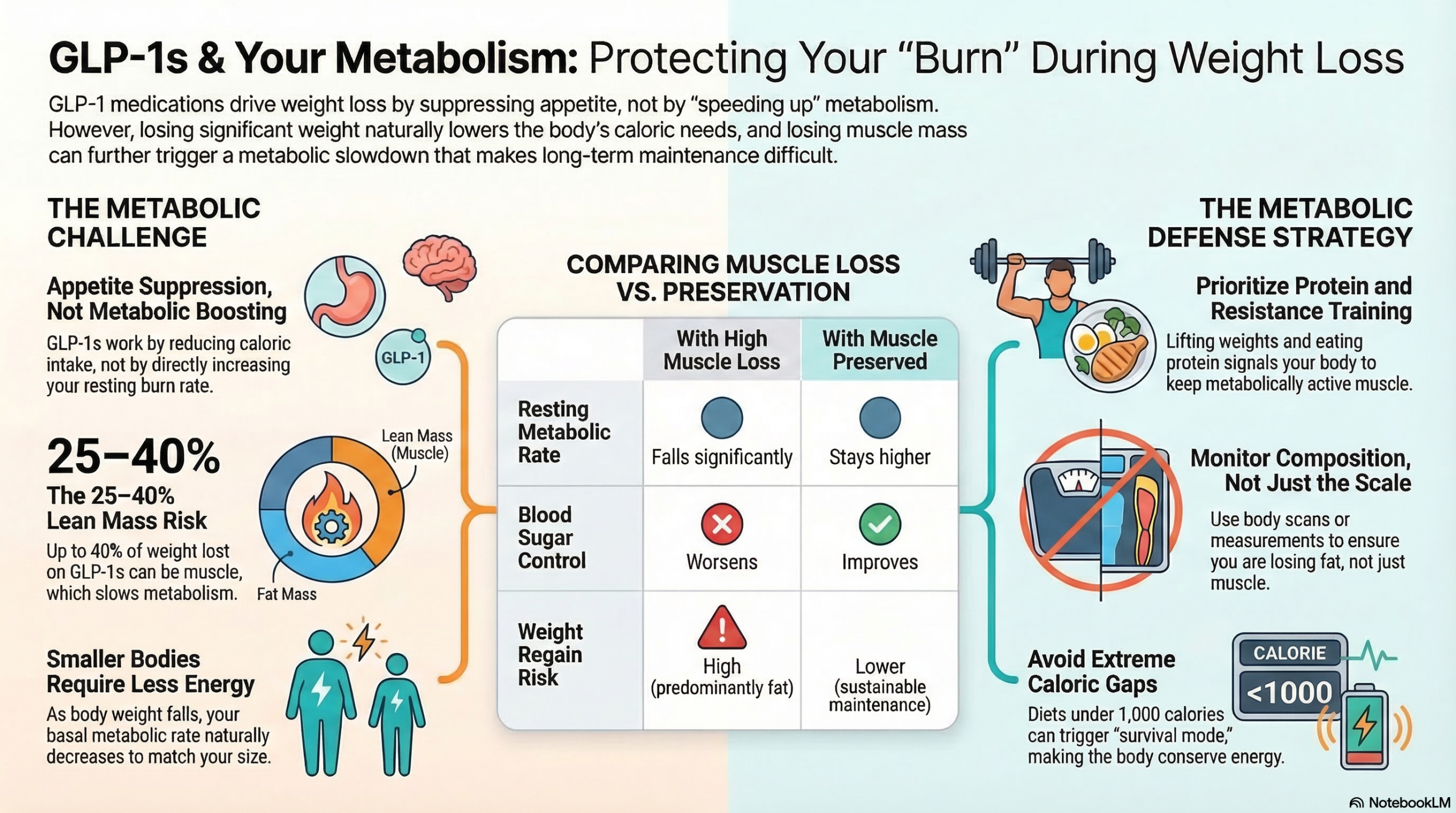
This is an important point to understand: GLP-1 drugs work by reducing how much you eat, not by directly speeding up how many calories you burn. The weight loss comes from the caloric deficit they create — not from any turbocharging of metabolism.
These drugs do not directly increase the speed of your metabolism. They do not increase how many calories your body burns at rest. Their primary mechanism is appetite suppression — creating a caloric deficit by reducing how much you eat. The metabolic effects of GLP-1 therapy are largely indirect consequences of the weight loss they produce.
4. Weight Loss and Metabolism
Here is a fact about metabolism that applies to every weight loss method — diet, exercise, surgery, or medication: when you lose weight, your body burns fewer calories than it did before. This is not a flaw or a side effect. It is a predictable biological response.
There are two main reasons for this:
First, a smaller body simply needs less energy. If you weigh 200 pounds, your body must work harder to move, breathe, and pump blood than if you weigh 160 pounds. As body weight falls, the caloric cost of existing — your basal metabolic rate — falls with it. This happens with every form of weight loss.
Second, the body adapts to caloric restriction. When calorie intake drops significantly, the body responds by becoming more efficient — essentially learning to do more with less. This process, called adaptive thermogenesis or metabolic adaptation, means that actual calorie burn may fall slightly more than would be predicted from body size alone. Researchers have studied this for decades and it is well-documented across multiple weight loss approaches, not just GLP-1 drugs.
The practical implication is this: after losing significant weight on a GLP-1 drug, you will need fewer calories per day to maintain your new weight than you needed to maintain your old weight. This is not a sign that something has gone wrong. It is normal physiology adjusting to a new body size.
The concern is what happens when the drug is stopped. Studies following people who discontinued semaglutide found that most regained a substantial portion of their weight within a year. This is partly because the appetite suppression disappears when the drug stops — but also because the body has adjusted to a lower caloric need, and previous eating habits produce a surplus again.
Research published in 2022 following STEP 1 trial participants who stopped semaglutide found that they regained approximately two-thirds of their lost weight within one year of stopping the drug. Critically, the regained weight was predominantly fat — not the muscle lost during treatment. This progressive worsening of body composition is one reason muscle preservation during active treatment matters so much.
5. The Role of Muscle in Metabolic Rate
Of all the factors that influence metabolic rate, skeletal muscle mass is the one you have the most control over. And it is directly at stake during GLP-1 therapy.
Muscle tissue is metabolically expensive. It burns significantly more calories per pound than fat tissue — both at rest and during activity. When you lose muscle, your resting metabolic rate falls. When you gain or maintain muscle, it stays higher.
Clinical trials have confirmed that 25–40% of weight lost on GLP-1 drugs may come from lean mass — which includes muscle. For someone losing 15 kg (33 pounds), that could mean 4–6 kg (9–13 pounds) of muscle lost. That is a significant metabolic consequence.
Metabolic Consequences
- Resting metabolic rate falls significantly
- Body burns fewer calories at rest
- Blood sugar control worsens
- Physical strength declines
- Higher risk of weight regain after stopping
- Harder to maintain weight loss long-term
Metabolic Advantages
- Resting metabolic rate stays higher
- Body continues burning more calories at rest
- Blood sugar control improves
- Physical strength maintained or improved
- Lower risk of fat-dominant weight regain
- Better foundation for long-term weight maintenance
This is why researchers and clinicians increasingly argue that muscle preservation should be a primary goal during GLP-1 therapy — not an afterthought. Protecting lean mass protects metabolism. And a better metabolism makes the long-term weight outcome — whether you stay on the drug or eventually stop — significantly more favorable.
More muscle = higher metabolic rate = more calories burned at rest = easier to maintain a healthy weight long-term. Losing muscle during GLP-1 therapy works directly against the goal of sustainable weight management, even if the scale shows good short-term results.
6. Do GLP-1 Drugs Slow Metabolism?
This is the question most people want answered directly. The honest answer is: not directly — but weight loss always does, and GLP-1 drugs produce a lot of weight loss.
Let's break that down into three parts.
GLP-1 drugs do not directly reduce how many calories your body burns. There is no evidence that semaglutide or tirzepatide directly suppress metabolic rate. They do not slow the thyroid, reduce mitochondrial activity, or otherwise directly lower energy expenditure. Their mechanism is appetite suppression — eating less, not burning less.
But weight loss from any cause reduces daily calorie burn. As described in Section 4, a smaller body burns fewer calories. This is unavoidable. After losing 15–20% of body weight on a GLP-1 drug, your daily calorie need is meaningfully lower than it was at your starting weight. This is not the drug slowing metabolism — it is your metabolism adjusting to your new body size.
And GLP-1-related muscle loss compounds the effect. When a significant fraction of weight lost is lean mass, the metabolic slowdown is greater than it would have been if that weight had been pure fat. This is the most preventable part of the metabolic equation — and the one most under your control.
- GLP-1 drugs do not directly slow metabolism — they suppress appetite and create a caloric deficit
- Losing significant body weight always lowers daily calorie requirements — this is basic physiology
- Losing muscle during weight loss compounds the metabolic slowdown beyond what body size alone explains
- The degree of metabolic slowdown depends heavily on how much muscle you preserve during treatment
- Long-term weight management after GLP-1 therapy is more successful when lean mass is protected during treatment
Some researchers also note that GLP-1 drugs may have modest positive effects on energy expenditure through mechanisms like increasing postmeal thermogenesis — the calorie burn that comes from digesting food — and improving insulin sensitivity, which affects how efficiently cells use energy. These effects are relatively small compared to the caloric restriction impact, but they suggest the metabolic picture is not entirely negative.
7. How to Support Healthy Metabolism
The good news is that the metabolic consequences of GLP-1 therapy are not fixed. There are clear, evidence-based strategies that can minimize metabolic slowdown during treatment and set you up for better long-term outcomes.
Prioritize Protein at Every Meal
Protein has the highest thermic effect of any macronutrient — your body burns more calories digesting protein than it does processing fat or carbohydrates. More importantly, adequate protein intake is essential for maintaining muscle mass during caloric restriction. Target 1.2–1.6 grams of protein per kilogram of body weight per day. When appetite is suppressed by a GLP-1 drug, plan protein-rich foods first at every meal so you secure this macronutrient before fullness sets in.
Do Resistance Training at Least Twice a Week
Resistance exercise — working muscles against a load, whether that is bodyweight, bands, or weights — sends a direct signal to the body to maintain and build muscle tissue. This is the most powerful tool available for counteracting GLP-1-related lean mass loss. Even two sessions per week of moderate resistance training significantly reduces muscle loss compared to no exercise. Beyond muscle preservation, resistance training independently boosts resting metabolic rate and improves insulin sensitivity.
Stay Physically Active Throughout the Day
Daily physical activity — walking, taking stairs, standing rather than sitting — contributes to what researchers call non-exercise activity thermogenesis (NEAT). This is a surprisingly large component of daily calorie burn that is easy to let slip during a period of low appetite and lower energy. Maintaining or increasing daily movement while on a GLP-1 drug helps counteract the reduction in total calorie expenditure that comes with weight loss.
Prioritize Sleep Quality
Sleep is one of the most underappreciated metabolic factors. Poor or insufficient sleep reduces the hormone that stimulates muscle building (growth hormone), increases the stress hormone cortisol (which promotes muscle breakdown), impairs insulin sensitivity, and increases hunger the following day. Adults taking GLP-1 drugs who sleep fewer than 7 hours per night may be compounding the metabolic challenges of caloric restriction. Consistent, high-quality sleep of 7–9 hours supports every aspect of metabolic health.
Monitor Body Composition, Not Just Weight
A scale tells you total body weight. It does not tell you how much of that weight is fat and how much is muscle. Two people can both lose 15 kg on a GLP-1 drug and have completely different metabolic outcomes depending on how much of that loss was lean mass. Tracking body composition — using a DXA scan, bioimpedance measurement, or even simple waist and arm circumference measurements — gives you the data to know whether your metabolism is being protected or eroded during treatment.
Avoid Extreme Caloric Restriction
GLP-1 drugs can suppress appetite so strongly that some people eat very little — sometimes fewer than 1,000 calories per day. While this accelerates short-term weight loss, extreme restriction accelerates muscle loss and metabolic adaptation. The body interprets severe caloric deficit as a survival threat and becomes increasingly efficient at conserving energy. A moderate deficit of 500–750 calories per day is generally considered optimal for preserving metabolic rate and lean mass while still losing fat at a meaningful pace.
8. Key Takeaways
Frequently Asked Questions
Not permanently in an irreversible sense — but it will be calibrated to your new, lower body weight. After losing significant weight, your body requires fewer calories to function than it did at your previous weight. This is true for all weight loss methods, not just GLP-1 drugs. If you regain weight after stopping the medication, your metabolic rate will generally rise again in proportion to the regained mass — though if that regained mass is mostly fat rather than muscle, the metabolic recovery will be less complete. The key is protecting muscle during treatment so the metabolic floor stays as high as possible.
There are two main reasons. First, the primary effect of GLP-1 drugs — appetite suppression — disappears when the drug is stopped. Hunger returns to pre-treatment levels, and without the hormonal brake on appetite, food intake rises back toward previous habits. Second, the body has adapted to a lower caloric need during the weight loss period. When appetite returns to normal and eating increases, the body is now in caloric surplus relative to its reduced metabolic rate, and weight regain follows. Research shows this is not unique to GLP-1 drugs — it is the consistent outcome when any appetite-suppressing treatment is discontinued without lifestyle changes in place to sustain the deficit independently.
Exercise does not meaningfully reduce the appetite-suppressing or blood sugar effects of GLP-1 drugs. The drugs work through hormonal mechanisms that are independent of physical activity. What exercise does change — significantly — is body composition during treatment. People who add resistance training to GLP-1 therapy lose substantially less muscle as a proportion of their total weight loss. This means their metabolic rate holds up better, their physical function improves, and their long-term weight maintenance prospects are stronger. Exercise also improves insulin sensitivity and cardiovascular health independently of the drug's effects.
Yes, adaptive thermogenesis is real and well-documented in caloric restriction research. It refers to the body burning slightly fewer calories than would be predicted based on body size alone — essentially adapting to the reduced caloric environment by becoming more efficient. This has been observed in people losing weight through various methods and is not unique to GLP-1 therapy. The effect is generally modest — on the order of 100–300 additional calories per day beyond what body size alone predicts — but it does contribute to why weight loss slows over time and why maintaining a deficit becomes progressively harder. The best mitigation is maintaining muscle mass through resistance training and adequate protein.
You cannot completely offset the metabolic reduction that comes with losing body mass. However, you can significantly minimize how much your resting metabolic rate falls by preserving or building muscle tissue during treatment. Regular resistance training — combined with adequate protein intake — stimulates muscle protein synthesis and maintains the metabolically active tissue that keeps resting calorie burn higher. Some research also shows that resistance training independently increases resting metabolic rate beyond just its muscle-preservation effect, through improvements in mitochondrial density and hormonal environment in muscle tissue. The goal is not to "boost" metabolism with tricks — it is to protect the primary determinant of metabolic rate, which is lean muscle mass.
The available evidence suggests that for people with obesity and related metabolic conditions — particularly type 2 diabetes and cardiovascular disease — the benefits of long-term GLP-1 therapy substantially outweigh the metabolic concerns described in this article. Large outcome trials like SELECT have shown significant reductions in major cardiovascular events in people taking semaglutide long-term. The metabolic considerations discussed here — muscle loss, metabolic adaptation — are real and worth managing proactively, but they are manageable through protein intake and exercise. They are not reasons to avoid GLP-1 therapy in people who have been prescribed it for appropriate clinical reasons. Always discuss the risks and benefits of long-term treatment with your prescribing physician.
-
1
Wilding JPH, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine. 2021;384(11):989–1002. doi.org/10.1056/NEJMoa2032183
-
2
Wilding JPH, et al. "Weight regain and cardiometabolic effects after withdrawal of semaglutide." Diabetes, Obesity and Metabolism. 2022;24(8):1553–1564. doi.org/10.1002/dom.14725
-
3
Neeland IJ, Linge J, Birkenfeld AL. "Changes in lean body mass with GLP-1-based therapies and mitigation strategies." Diabetes, Obesity and Metabolism. 2024;26(Suppl 4):16–27. doi.org/10.1111/dom.15728
-
4
Rosenbaum M, Leibel RL. "Adaptive thermogenesis in humans." International Journal of Obesity. 2010;34(Suppl 1):S47–55. doi.org/10.1038/ijo.2010.184
-
5
Linge J, Birkenfeld AL, Neeland IJ. "Muscle mass and GLP-1 receptor agonists: adaptive or maladaptive?" Circulation. 2024. doi.org/10.1161/CIRCULATIONAHA.124.067676
-
6
Lichtman SW, et al. "Discrepancy between self-reported and actual caloric intake and exercise in obese subjects." New England Journal of Medicine. 1992;327(27):1893–1898. doi.org/10.1056/NEJM199212313272701
