
Building Strength at 60+: The Role of C10 Triglycerides
Most strength research was done on young, healthy adults. A decade-long Japanese clinical trial series tested something different — what happens when frail adults averaging age 85 take just 6 grams of C8/C10 MCTs per day for 90 days. The results were measurable, significant, and directly applicable to everyone over 60.
If you are over 60, the single most important nutritional investment you can make is in your muscle tissue. Not for aesthetics — for independence, fall prevention, metabolic health, and survivability. And the gap between what most people do about it and what the research supports is enormous.
The supplement industry has been loud about protein powders, creatine, and branched-chain amino acids for muscle building. These are legitimate tools — but they were developed for younger athletes, not for adults whose mitochondria are aging, whose carnitine levels are declining, and whose muscle cells are fighting a losing biochemical battle against decades of accumulated cellular fatigue.
This article focuses on what a specific body of clinical research — built over more than a decade by a team at Showa Women's University in Tokyo — says about the measurable effects of C8/C10 medium-chain triglycerides on muscle mass, strength, and function in adults averaging age 85 years old. If it works there, it works for you.
What Actually Happens to Muscle After 60
Sarcopenia — the progressive age-related loss of skeletal muscle mass and function — is not a dramatic cliff-edge event. It is a slow, invisible erosion that begins in your 30s and accelerates with each passing decade. By the time most people notice it, they have already lost a significant fraction of the muscle tissue they had at peak mass.
The Silent Start
Longitudinal studies show measurable muscle mass and strength decline begins around age 35, primarily in fast-twitch Type II muscle fibers — the fibers responsible for power, speed, and catching yourself from a fall.
1–2% Loss Per Year Begins
After age 50, muscle mass decreases at roughly 1–2% per year and strength declines at 1.5% annually. This compounds: someone who loses 1.5% per year from age 50 to 70 has lost approximately 26% of that starting baseline over two decades.
Acceleration — Strength Drops 3%/Year
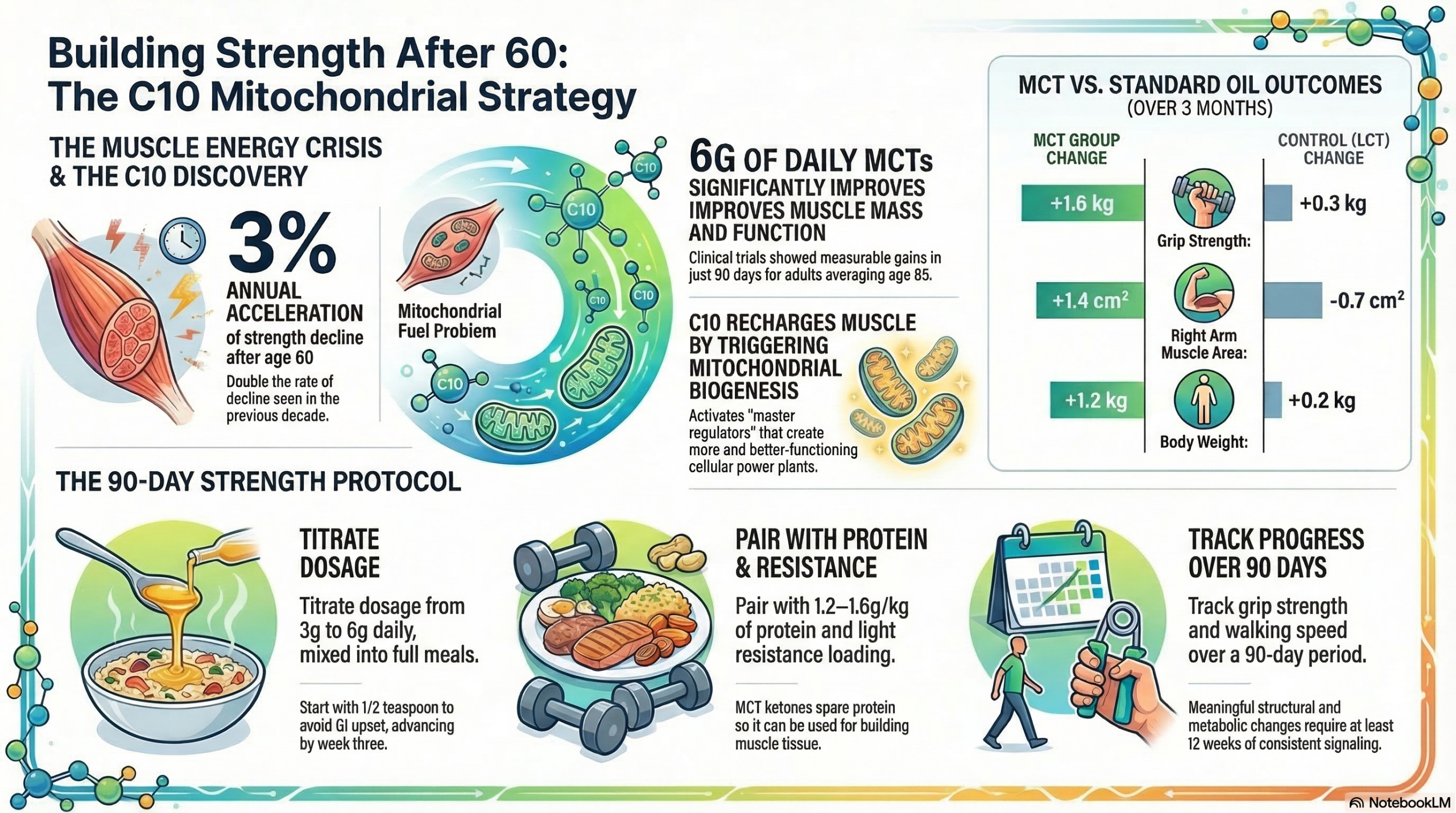
After 60, the rate of strength decline accelerates to ~3% per year — double the rate of the prior decade. Between 5 and 13% of adults aged 60–70 meet clinical criteria for sarcopenia. Mitochondrial dysfunction, declining anabolic hormone levels, and reduced GH secretion all converge.
Prevalence Reaches 11–50%
By age 80, between 11% and 50% of adults have clinically significant sarcopenia depending on diagnostic criteria. Falls, fractures, loss of independence, cognitive decline, and mortality risk all climb in direct proportion to muscle loss severity.
The conventional response to sarcopenia is resistance training plus protein supplementation. Both are well-supported and important. But they address the structural side of muscle building — not the cellular energy deficit that is the root cause of why aging muscle recovers more slowly and responds less robustly to training in the first place. This is where C10 enters the picture.
Aging skeletal muscle is not primarily a protein problem. It is a mitochondrial fuel problem. The mitochondria in aging muscle cells are fewer, less efficient, and more prone to oxidative damage than in younger tissue. When muscle cells cannot produce enough ATP to fuel the contractile machinery, muscle protein breaks down faster than it is synthesized — regardless of how much protein is in the diet. C10 addresses this root cause by rebuilding and recharging the mitochondrial machinery itself.
The Clinical Evidence: What the Ezaki & Abe Trial Series Found
Between 2016 and 2023, researchers Sakiko Abe and Osamu Ezaki at Showa Women's University conducted three randomized controlled trials and a combined data analysis examining the effects of C8/C10 MCT supplementation on frail older nursing home residents. This is the most rigorous and specific human clinical dataset for C10 and muscle outcomes in aging adults.
In the combined analysis of two randomized trials (n = 29 MCT group, n = 27 LCT control group), supplementation with just 6g/day of C8/C10 MCTs at dinnertime for 3 months produced statistically significant improvements across multiple muscle and function measures compared to an equivalent dose of long-chain triglycerides. Key outcomes (MCT vs. LCT, adjusted mean change from baseline):
The MCTs were mixed directly into food (steamed rice or miso soup) at dinner — not taken as a shake or pill. The dose was 6g, roughly 1–1.5 teaspoons. No other exercise or nutritional changes were required. The authors concluded that MCTs represent a practical, daily-life tool for treating sarcopenia in older adults.
Why These Results Matter — Even If You're Not 85
The participants in this trial series were among the most physiologically challenged test population imaginable for muscle intervention: frail nursing home residents with a mean age of 85, limited mobility, and likely compromised mitochondrial function across multiple organ systems. If a 6g/day supplement can produce significant, measurable gains in this population, it represents a genuine floor — not a ceiling — of what C10 can do for active adults in their 60s and 70s with more intact baseline muscle biology.
The fact that results reached significance in a combined sample of just 56 participants is noteworthy. Small-sample studies are typically underpowered to detect real effects — which means the underlying signal in this data is likely substantial. The researchers themselves noted that individual trials fell short of significance partly due to sample size, not effect strength.
These trials used C8/C10 mixed MCTs, not pure C10 Tricaprin alone. The relative contribution of C8 vs. C10 to the observed muscle outcomes has not been fully disentangled in human studies. The mechanistic research (PPARγ, GLP-1, mitochondrial biogenesis) points to C10 as the more active molecule for muscle and metabolic effects — but the human outcome data is derived from a blend. Additionally, the trial populations were institutionalized frail elderly adults; results in community-dwelling adults at 60–70 with higher baseline function may differ.
Three Mechanisms That Explain the Results
Following the publication of the 2023 combined analysis, Ezaki published a 2024 follow-up paper in Nutrients specifically asking: what are the extracellular signals that explain how MCTs produce these muscle outcomes? Three leading hypotheses emerged from the mechanistic literature, each well-supported by preclinical data.
Mechanism 1: Sympathetic Nervous System Activation → PGC-1α → Mitochondrial Biogenesis
C10 increases postprandial energy expenditure via stimulation of the sympathetic nervous system (SNS). SNS activation triggers beta-2 adrenergic receptor signaling in muscle cells, which acutely upregulates isoforms of PGC-1α — the master regulator of mitochondrial biogenesis — and chronically induces muscle hypertrophy over approximately 30 days. This is a carnitine-independent upstream signal: C10 doesn't need to enter the mitochondria itself to initiate this cascade; it initiates it systemically through the SNS-adrenergic axis.
Mechanism 2: Acyl-Ghrelin Elevation → Growth Hormone Secretion
C10 at even low doses (as little as 3g) has been shown to increase plasma acyl-ghrelin — the active, hunger-stimulating form of ghrelin that also potently stimulates growth hormone (GH) release. Because GH secretion declines significantly with aging, and because GH drives muscle protein synthesis, this acyl-ghrelin → GH pathway may be particularly valuable for older adults whose natural GH axis has become sluggish. C10's ability to partially reactivate this hormonal anabolic signal through a dietary mechanism — without exogenous GH — is a distinct advantage.
Mechanism 3: Ketone Bodies as Nitrogen-Sparing Muscle Fuel
C10 is metabolized by the liver into ketone bodies, which skeletal muscle can use as a direct fuel source. When muscle cells have access to ketones, they oxidize less protein for energy — a phenomenon called the nitrogen-sparing effect. In malnourished or low-calorie conditions (which is common in frail elderly adults), this means more dietary protein is preserved for muscle protein synthesis rather than burned as fuel. The net result is an improved muscle protein balance: the same dietary protein produces more net muscle tissue when ketones are also present as a competing energy substrate.
These three mechanisms operate in parallel and are additive. They explain why 6g/day — a dose that sounds trivially small — can produce meaningful results across multiple strength and mass measures in just 90 days. C10 is not adding fuel to a tank; it is reactivating the signaling systems that tell aging muscle to grow and recover.
The Research Foundation
The Primary Clinical Article — Ezaki & Abe 2023
The combined data analysis of three clinical trials confirming that 6g/day of C8/C10 MCTs over 3 months significantly increased body weight, arm muscle area, calf circumference, grip strength, walking speed, and knee extension time in frail adults (mean age 85) — while decreasing fat mass. This is the strongest and most directly applicable human clinical evidence for C10 and muscle outcomes in aging populations.
Read the Study → Frontiers in Nutrition, 2023Mechanistic Follow-Up: Extracellular Signals Behind the Results — Ezaki 2024
Published in Nutrients (August 2024), this review by Ezaki specifically addresses the question of how MCTs produce muscle outcomes — proposing the SNS/PGC-1α axis, acyl-ghrelin/GH secretion, and ketone nitrogen-sparing as the three primary extracellular mechanisms. This paper provides the biological explanation for why the 2023 clinical findings occurred and guides future clinical trial design.
Read the Study → Nutrients, August 2024C10 PPARγ Activation & Mitochondrial Biogenesis — Hughes et al. 2014
This foundational cell-line study demonstrated that C10 — specifically, not C8 — activates PPARγ and increases mitochondrial citrate synthase and Complex I activity in neuronal cells. PPARγ is upstream of PGC-1α, making this study the mechanistic anchor connecting C10 intake to the mitochondrial biogenesis cascade that ultimately produces more and better-functioning mitochondria in muscle tissue.
Read the Study → Journal of Neurochemistry, 2014Sarcopenia Epidemiology: 10–16% of Older Adults Globally — Yuan & Larsson 2023
This systematic review in Metabolism (Karolinska Institutet) established that sarcopenia affects 10–16% of elderly adults worldwide and is associated with falls, fractures, cognitive impairment, metabolic disorders, and increased mortality. Muscle strength declines at 1.5% per year from ages 50–60, accelerating to 3% per year thereafter. This context establishes why the Ezaki & Abe clinical findings are not a niche concern — sarcopenia is one of the most prevalent and consequential aging conditions globally.
Read the Study → Metabolism, 2023Tricaprin Corrects Cellular Energy Failure in Muscle Tissue — Hirano et al. 2025
The Nature Cardiovascular Research 2025 registry study documenting 100% 3-year survival in TGCV heart failure patients treated with Tricaprin establishes that C10's ability to restore intracellular fat metabolism extends to the most demanding muscle tissue in the body: the cardiomyocyte under conditions of complete metabolic failure. This represents a proof-of-concept for C10's ability to rescue energy production in muscle cells when endogenous fat metabolism has broken down.
Read the Study → Nature Cardiovascular Research, 2025C10 Respiratory Chain Enhancement — Viswanath et al. 2020
This Nutrients study demonstrated that C10 upregulates mitochondrial respiratory chain Complexes I and II, increases SIRT1 activity (the longevity enzyme), and enhances overall oxidative phosphorylation efficiency. In aging skeletal muscle where Complex I activity is known to decline with age, C10's ability to upregulate this specific complex represents a targeted intervention at the site of age-related mitochondrial decline.
Read the Study → Nutrients, 2020The 90-Day Strength Protocol for Adults 60+
The following protocol is drawn directly from the Ezaki & Abe trial series parameters, adjusted for real-world use by adults 60–80 who are more mobile and metabolically capable than the nursing home participants in the trials. Consider these recommendations a conservative lower bound — the trial produced significant results in far more compromised subjects.
Start at 3g C10 Per Day — Scale to 6g at Week 3
The Ezaki trials used 6g/day, but starting there can cause GI discomfort in MCT-naive adults. Begin with approximately half a teaspoon of C10-rich MCT oil or pure Tricaprin (≈3g) mixed into a meal. At weeks 2–3, advance to the full 6g/day used in the trial. This gradual titration reduces GI adjustment effects and improves long-term adherence.
📋 Trial Protocol: 6g/day at dinnerTake C10 With a Full Meal — Not a Snack or on an Empty Stomach
In all three Ezaki & Abe trials, MCTs were mixed directly into food at dinnertime — specifically with calorie-dense foods like steamed rice or miso soup. The meals provided the metabolic substrate context that allowed GLP-1 release, acyl-ghrelin stimulation, and optimal liver processing of C10 into acylcarnitine for downstream muscle delivery. Taking C10 in isolation or with a very small snack reduces the hormonal cascade it is intended to trigger.
🍚 Mixed into food — not taken as a capsule alonePair With Adequate Protein — 1.2–1.6g per kg Bodyweight
C10's nitrogen-sparing mechanism works by providing an alternative fuel (ketones) so that dietary protein is allocated to synthesis rather than burned for energy. But this only matters if there is adequate dietary protein present. For adults 60+, current evidence supports 1.2–1.6g of protein per kilogram of bodyweight per day — significantly above the outdated 0.8g/kg RDA. C10 amplifies the productivity of protein; it does not replace it.
🥚 Protein target: 1.2–1.6g/kg/dayAdd Any Form of Resistance Loading — Even Minimal
C10 triggers PGC-1α via the SNS-adrenergic axis; resistance exercise triggers it via the AMPK pathway. These are two independent, additive signals for mitochondrial biogenesis and muscle protein synthesis. The bar for meaningful resistance loading at 60+ is low: bodyweight squats, wall push-ups, resistance bands, stair climbing, or light dumbbell work 2–3× per week is sufficient to compound on C10's cellular signals. The Ezaki trial showed results with no required exercise protocol — imagine the results with a light training program added.
🏋️ Even 2× weekly resistance work is additiveTrack These Three Markers at Baseline and Week 12
The Ezaki trials tracked grip strength, walking speed, and limb circumference. These are accessible and meaningful. At baseline: measure dominant hand grip strength using a simple dynamometer (available on Amazon for under $20), time your walking speed over a 10-meter course, and measure your dominant arm circumference at mid-bicep. Repeat at 12 weeks. These are the exact markers the clinical trials used — and they will tell you more than the scale will.
📏 Grip strength · Walking speed · Arm circumferenceCommit to 90 Days Before Evaluating
The Ezaki & Abe trials ran for exactly 3 months. Mitochondrial biogenesis, GH axis reactivation, and nitrogen balance improvements are structural and metabolic changes that require consistent signaling over weeks — not acute effects you will feel after a single dose. Muscle area changes (+1.4 cm² arm muscle area in the trial) take time to accumulate. Set a calendar reminder for your 90-day assessment and focus on consistency rather than early subjective effects.
🗓️ 90-day minimum before evaluating results-
1
Primary Clinical Article — MCTs Increase Muscle Mass & Function in Frail Older Adults — Ezaki O, Abe S. "Medium-chain triglycerides (8:0 and 10:0) increase muscle mass and function in frail older adults: a combined data analysis of clinical trials." Frontiers in Nutrition. 2023;10:1284497.
DOI: https://doi.org/10.3389/fnut.2023.1284497 -
2
Mechanistic Follow-Up: Extracellular Signals Behind MCT Muscle Effects — Ezaki O. "Possible Extracellular Signals to Ameliorate Sarcopenia in Response to Medium-Chain Triglycerides (8:0 and 10:0) in Frail Older Adults." Nutrients. 2024;16(16):2606.
DOI: https://doi.org/10.3390/nu16162606 -
3
C10 PPARγ Activation & Mitochondrial Biogenesis — Hughes SD, Kanabus M, Anderson G, et al. "The ketogenic diet component decanoic acid increases mitochondrial citrate synthase and complex I activity in neuronal cells." Journal of Neurochemistry. 2014;129(3):426–433.
DOI: https://doi.org/10.1111/jnc.12646 -
4
C10 Respiratory Chain & SIRT1 Activation — Viswanath G, et al. "Decanoic acid and not octanoic acid stimulates fatty acid synthesis..." Nutrients. 2020;12(8):2379.
DOI: https://doi.org/10.3390/nu12082379 -
5
Sarcopenia Epidemiology: Prevalence, Risk Factors & Consequences — Yuan S, Larsson SC. "Epidemiology of sarcopenia: Prevalence, risk factors, and consequences." Metabolism. 2023;144:155533.
DOI: https://doi.org/10.1016/j.metabol.2023.155533 -
6
Tricaprin Long-Term Survival in TGCV Heart Failure — Hirano K, et al. "Long-term survival and durable recovery of heart failure in patients with triglyceride deposit cardiomyovasculopathy treated with tricaprin." Nature Cardiovascular Research. 2025;4(3):266–274.
DOI: https://doi.org/10.1038/s44161-025-00611-7
