
How to Preserve Muscle While Taking GLP-1 Weight-Loss Drugs
GLP-1 medications can cause significant muscle loss alongside fat loss. Science shows that protein and resistance training can protect lean mass — here is what you need to know.
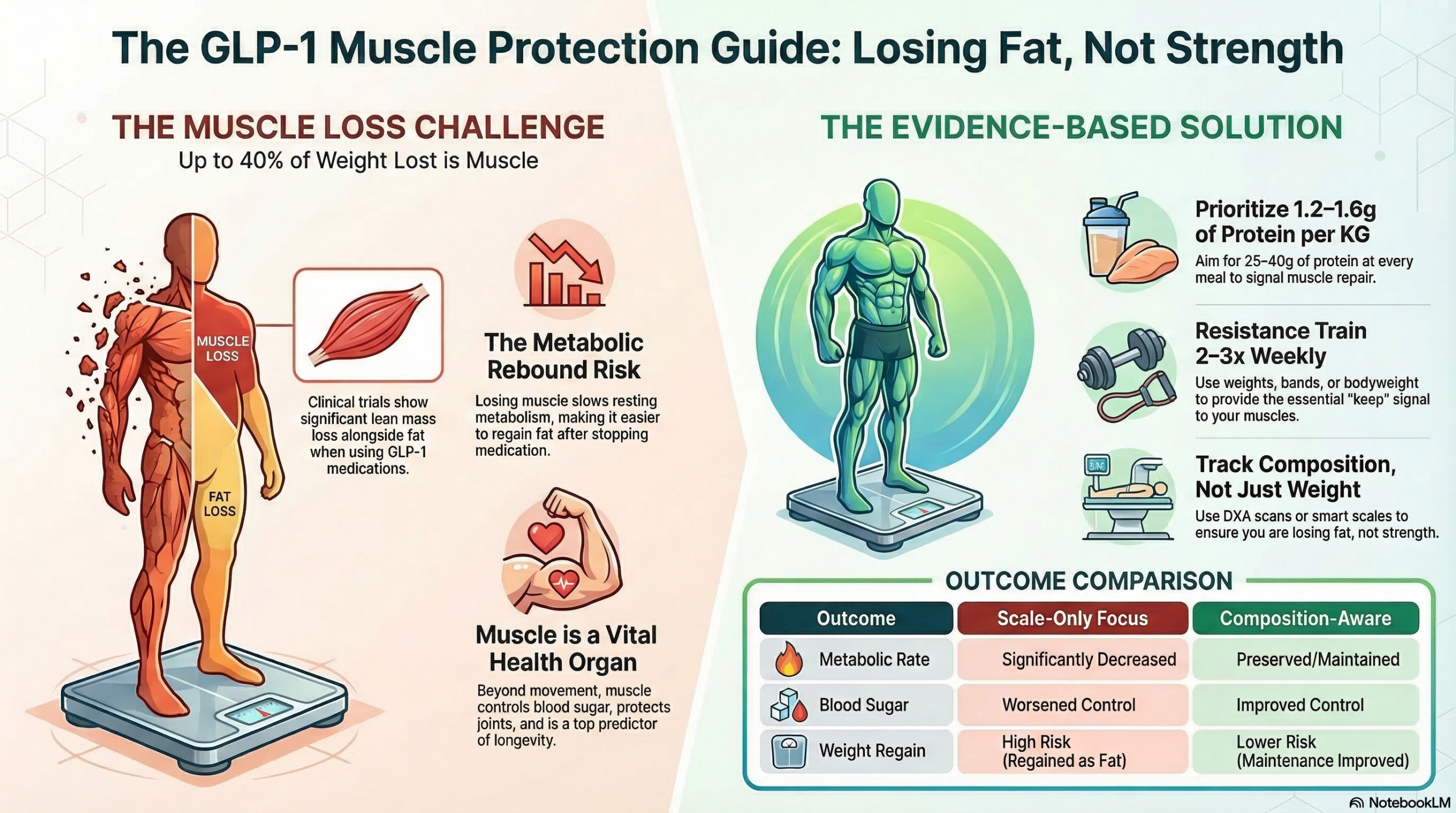
GLP-1 receptor agonist drugs — like semaglutide and tirzepatide — are highly effective for weight loss, but clinical trials show that 25–40% of the weight lost can come from muscle, not just fat. This article explains why muscle matters, what the research shows about lean mass loss on these drugs, and the evidence-based strategies — protein intake, resistance exercise, and smart monitoring — that can help protect your muscle while losing weight.
1. Introduction
GLP-1 receptor agonist drugs have changed how millions of people approach weight loss. Medications like semaglutide (sold as Ozempic and Wegovy) and tirzepatide (Mounjaro and Zepbound) help people lose significant amounts of weight — often 15–20% of their body weight over about a year.
That is a remarkable result. But weight on the scale is not the whole story.
Clinical trials have consistently shown that when people lose weight on these drugs, a meaningful portion of what they lose is not fat — it is muscle. Researchers estimate that anywhere from 25% to 40% of total weight lost on GLP-1 drugs may come from lean mass, which includes skeletal muscle.
Losing muscle while losing fat creates a problem. Muscle does far more than make you look fit. It protects your joints, supports your metabolism, helps your body use blood sugar, and plays a direct role in how long and how well you live. Losing a significant amount of it during weight loss can undermine many of the health benefits you were trying to achieve in the first place.
The good news is that this muscle loss is not inevitable. Research points to clear, practical strategies that can protect lean mass during GLP-1 therapy. This article explains what those strategies are and why they work.
The cardiovascular and metabolic benefits of semaglutide and tirzepatide are well-documented and, for many people, life-changing. This article is about making GLP-1 therapy work better — not about avoiding it. Protecting muscle mass during weight loss is a goal that every person on these medications should know about.
2. Why Muscle Matters During Weight Loss
Most people think of muscle as something athletes care about. In reality, muscle tissue is one of the most important organs in your body — and everyone, at every age, depends on it.
Here is what skeletal muscle does for you that most people do not realize:
- Burns calories at rest. Muscle is metabolically active tissue. The more you have, the more energy your body uses even when you are sitting still. Losing muscle lowers your resting metabolic rate, making it harder to keep weight off long-term.
- Controls blood sugar. Skeletal muscle is the body's largest site for glucose uptake. When you eat carbohydrates, muscle absorbs most of the glucose. Less muscle means less capacity to clear blood sugar — which matters enormously for people with or at risk of type 2 diabetes.
- Prevents falls and fractures. Muscle strength is the primary defense against falls in older adults. Falls are a leading cause of disability and death after age 65. Losing muscle accelerates this risk.
- Supports long-term weight maintenance. People who lose muscle during weight loss are more likely to regain weight afterward — because their metabolism has slowed and their body composition has worsened.
- Predicts longevity. Studies have consistently found that grip strength and muscle mass are among the strongest predictors of healthy aging and reduced mortality risk.
Muscle loss with aging — called sarcopenia — already happens naturally. After age 60, adults can lose 1–3% of their muscle strength every year without any intervention. Adding significant GLP-1-driven muscle loss on top of natural age-related decline can accelerate a process that was already working against you.
Older adults already have lower muscle protein synthesis rates and reduced anabolic (muscle-building) hormone levels. They are more vulnerable to GLP-1-related lean mass loss than younger adults — and the consequences are more serious. If you are over 55 and starting a GLP-1 drug, muscle preservation should be a primary goal of your treatment plan, not an afterthought.
3. What Studies Show About Muscle Loss on GLP-1 Drugs
The evidence on lean mass loss during GLP-1 therapy comes from the same large clinical trials that established these drugs as effective for weight loss. The body composition data was collected in subgroups of trial participants using a technique called DXA scanning — a precise way to measure fat, muscle, and bone separately.
To put those numbers in everyday terms: a person who loses 15 kilograms (about 33 pounds) on semaglutide may have lost 4–6 kilograms of that as muscle. That is roughly equivalent to 8–13 pounds of lean mass — the kind of loss that would typically take years of aging to accumulate naturally through sarcopenia.
Why does this happen? GLP-1 drugs work by suppressing appetite. When you eat significantly less food, your body must find energy from somewhere. It pulls from both fat stores and muscle tissue. Without specific steps to protect muscle — eating enough protein and doing resistance exercise — the body has no strong signal to preserve its lean mass during rapid weight loss.
Research shows that when people stop taking GLP-1 drugs, they tend to regain weight — and most of what comes back is fat, not muscle. This means someone who loses 10 kg of mixed fat and muscle on the drug, then regains 10 kg after stopping, ends up with worse body composition than when they started. Protecting muscle during the treatment period is not just about now — it determines what happens if and when the drug is stopped.
4. Protein Intake and Muscle Preservation
Of all the things you can do to protect muscle while losing weight, eating enough protein is the most important. This is true for everyone — but it is especially critical for people on GLP-1 drugs, because these medications reduce appetite and total food intake. When you eat less overall, protein intake tends to fall significantly unless you make a deliberate effort to prioritize it.
Here is the basic science: muscle is made of protein. When you eat protein, your body breaks it down into amino acids and uses them to repair and build muscle tissue. If you do not eat enough protein, your body draws on muscle itself for the amino acids it needs — which is muscle loss.
How much protein do you need? The standard government recommendation for adults is 0.8 grams of protein per kilogram of body weight per day. However, research on weight loss and aging strongly suggests this is not enough. Most studies on muscle preservation during caloric restriction support a target of 1.2 to 1.6 grams of protein per kilogram of body weight per day — and some researchers recommend up to 2.0 grams for older adults or those doing resistance training.
For a 180-pound (82 kg) person, that means roughly 100–130 grams of protein per day. This requires deliberate planning — especially on a GLP-1 drug that makes eating feel difficult.
When appetite is suppressed, people naturally tend to eat less of everything — including protein. A simple strategy: at every meal, eat your protein source first, before anything else. This way, even if you feel full quickly, you have already secured the most important macronutrient for muscle maintenance.
Here are some high-protein foods that are easy to eat in smaller portions — important for people whose appetite is reduced:
Protein shakes and powders are a valid option when whole food intake is difficult due to nausea or low appetite — common side effects during the early weeks of GLP-1 therapy. They are not necessary, but they are useful if whole food protein is not achievable.
5. Resistance Training and Strength
If protein is the raw material for muscle, resistance training is the signal that tells your body to use it. Without a reason to keep muscle tissue, the body will sacrifice it during a caloric deficit. Resistance exercise is how you give your body that reason.
Resistance training does not mean you need to join a gym or lift heavy weights. The term simply means any exercise where your muscles work against a force — whether that is gravity, a resistance band, your own body weight, or a dumbbell. The key is progressive loading: gradually increasing the challenge over time so the muscles continue to receive a growth and maintenance stimulus.
Research consistently shows that resistance training during caloric restriction significantly reduces lean mass loss compared to caloric restriction alone. In some studies, people doing resistance training while losing weight maintained or even increased lean mass while still losing fat.
| Exercise Type | Examples | Muscle Signal | Equipment Needed |
|---|---|---|---|
| Bodyweight | Squats, push-ups, lunges, wall sits | Strong | None |
| Resistance Bands | Rows, presses, bicep curls, leg extensions | Strong | Bands ($10–20) |
| Free Weights | Dumbbell presses, deadlifts, rows | Very strong | Dumbbells |
| Machines | Leg press, chest press, lat pulldown | Very strong | Gym access |
| Cardio only (walking, cycling) | Brisk walking, stationary bike, swimming | Weak for muscle preservation | Minimal |
How often? Two to three resistance training sessions per week is the minimum supported by evidence for meaningful muscle preservation. Each session does not need to be long — 20 to 30 minutes of focused effort is enough to provide the muscle-preservation signal the body needs.
Start Simple — Bodyweight Is Enough to Begin
You do not need equipment, a gym membership, or a personal trainer to start resistance training. A set of bodyweight squats, wall push-ups, and standing lunges done 2–3 times per week provides a meaningful muscle-preservation signal. The goal in the first month is simply consistency — establishing the habit before adding complexity.
🏠 No gym required to startFocus on the Large Muscle Groups
The largest muscle groups — legs, back, and chest — produce the strongest metabolic and hormonal response when trained. Exercises like squats, lunges, rows, and presses recruit many muscles at once and give you more return for your effort than isolated movements like bicep curls. Prioritize multi-joint exercises that involve the lower body.
🦵 Legs + back + chest = most impactProgress Gradually — Make It Harder Over Time
Muscle adapts to whatever challenge you give it. If you do the same exercises at the same intensity forever, the signal to maintain muscle weakens. Add a small amount of difficulty every 2–3 weeks — one more repetition, a slightly heavier band, or a more challenging variation of the exercise. This principle is called progressive overload, and it is the core mechanism behind all effective resistance training.
📈 Slightly harder every 2–3 weeksTime Protein Near Your Workouts
Muscle protein synthesis — the process of building and repairing muscle — is elevated for several hours after resistance exercise. Consuming protein within 1–2 hours of a training session takes advantage of this window. It does not need to be a protein shake; a Greek yogurt, a chicken breast, or two boiled eggs work just as well. The timing amplifies the muscle-preservation effect of the training session.
🥚 Protein within 2 hours of training6. Nutritional Considerations
Beyond protein, there are several other nutritional factors that support muscle preservation during GLP-1 therapy. None of these are complicated — but they are easy to overlook when appetite is suppressed and overall food intake is low.
Total calorie intake should not drop too fast. GLP-1 drugs can reduce appetite dramatically — to the point where some people eat very little for weeks at a time. Extreme caloric restriction accelerates muscle loss. A moderate deficit of 500–750 calories per day is generally considered appropriate for sustainable fat loss without excessive lean mass sacrifice. If you find you are eating fewer than 1,200 calories per day (for women) or 1,500 (for men) consistently, speak with a registered dietitian.
Spread protein across the day. Muscle protein synthesis responds to individual protein doses — not just daily totals. Research suggests that eating 25–40 grams of protein at each meal is more effective for muscle maintenance than eating a small amount at breakfast and lunch and a large amount at dinner. Three protein-containing meals per day is a reasonable target.
Do not neglect micronutrients. When total food intake falls significantly, it becomes easy to fall short on vitamins and minerals that support muscle function. Vitamin D and calcium are critical for muscle contraction and bone health. Magnesium plays a role in muscle recovery. If your diet is significantly restricted, a basic multivitamin and vitamin D supplement may be worth discussing with your doctor.
Stay hydrated. GLP-1 drugs can cause nausea and vomiting in some people, which increases the risk of dehydration. Muscle is approximately 75% water. Even mild dehydration impairs muscle function and recovery. Aim for consistent fluid intake throughout the day — not just when thirsty.
Eat enough protein at every meal. Do not let your total daily calories drop so low that your body has no choice but to consume muscle for fuel. Train your muscles at least twice a week. These three steps, done consistently, address the core mechanisms of GLP-1-related lean mass loss.
7. Why Body Composition Matters More Than Scale Weight
The scale tells you your total body weight. It does not tell you how much of that weight is fat and how much is muscle. This distinction matters enormously — and it is often completely ignored in how GLP-1 therapy is monitored.
Consider two people who both lose 15 kilograms on a GLP-1 drug:
Lost 15 kg — but poorly
- 10 kg fat lost
- 5 kg muscle lost
- Metabolic rate has fallen
- Blood sugar control worsened
- Higher fall risk than before
- Weight regain likely — as fat
Lost 15 kg — and well
- 14 kg fat lost
- 1 kg muscle lost (or neutral)
- Metabolic rate preserved
- Blood sugar control improved
- Strength maintained or increased
- Better long-term weight maintenance
Both people lost the same amount of weight by the scale. But their health outcomes are dramatically different. Person B achieved what researchers call "high-quality weight loss" — predominantly fat, with lean mass protected.
How do you measure body composition? The most accurate method available to most people is a DXA scan. These are available at many radiology centers, university health facilities, and some fitness centers. A basic DXA scan costs $50–150 and gives you precise measurements of fat mass, lean mass, and bone density.
If a DXA scan is not accessible, bioelectrical impedance analysis (BIA) — available in many smart scales and at gyms — provides a reasonable estimate. It is less accurate than DXA but is far better than relying on scale weight alone. Simple measurements like waist circumference and mid-arm circumference, tracked over time, also give useful information about fat and muscle trends.
Most GLP-1 prescribers track weight, blood pressure, and metabolic labs at follow-up visits. Fewer routinely monitor body composition. Before starting a GLP-1 drug, consider asking: "How are we going to track my muscle mass during treatment?" Getting a baseline DXA scan before starting and repeating it every 3–6 months gives you data that a standard scale cannot provide.
8. Safety and Medical Guidance
Everything in this article is educational. None of it replaces the guidance of a physician, registered dietitian, or certified exercise professional. Before making changes to your diet or starting a new exercise program — especially if you are on a GLP-1 drug or have existing health conditions — speak with your healthcare team.
- Do not stop your GLP-1 medication because of concerns about muscle loss without discussing it with your doctor first. The cardiovascular and metabolic benefits of these drugs are substantial for many patients.
- High protein intake is safe for most adults but should be discussed with a physician if you have kidney disease, as high protein diets can affect kidney function in people with pre-existing kidney impairment.
- Start resistance training gradually if you are new to exercise — especially if you have joint issues, cardiovascular disease, or are significantly deconditioned. A brief consultation with a physical therapist or certified trainer can help you start safely.
- GLP-1 drugs slow gastric emptying, which means food and supplements stay in the stomach longer. This can affect when you feel hungry or full, and may require timing adjustments for protein intake and exercise.
- Older adults should be especially proactive — the lean mass risks on GLP-1 drugs are amplified in people over 60. Nutritional and exercise support should be integrated into GLP-1 prescribing for this population, not left to the patient to figure out independently.
A growing number of healthcare providers — endocrinologists, obesity medicine specialists, and registered dietitians — now offer integrated GLP-1 programs that include nutrition counseling and exercise guidance alongside the medication itself. If your current prescriber does not offer this, asking for a referral to a registered dietitian who specializes in obesity medicine is a reasonable step.
9. Key Takeaways
Frequently Asked Questions
Not necessarily — but the risk is real and significant without active countermeasures. Clinical trial data shows that lean mass loss occurs in most participants on semaglutide and tirzepatide, with estimates ranging from 25% to 40% of total weight lost. However, case series using DXA monitoring show that people who prioritize protein intake and resistance training can dramatically reduce or even eliminate lean mass loss while still losing substantial fat. The outcome depends largely on what you do alongside taking the medication.
Most research on weight loss and muscle preservation in adults supports a protein target of 1.2 to 1.6 grams per kilogram of body weight per day — significantly higher than the standard government recommendation of 0.8 g/kg. For a 175-pound (80 kg) person, that means roughly 96 to 128 grams of protein per day. Because GLP-1 drugs suppress appetite, you may need to plan meals deliberately around protein-rich foods, eat protein first at every meal, and potentially use protein supplements when whole food intake is challenging.
Start with bodyweight exercises at home — no gym, no equipment, no prior experience required. A basic routine of squats, wall push-ups, standing lunges, and a seated row using a resistance band covers the major muscle groups. Aim for 2 sessions per week to start, doing 2–3 sets of 10–15 repetitions of each exercise. If you have any joint problems, heart conditions, or have been sedentary for several years, a brief check-in with your doctor before starting is wise. Consider one or two sessions with a certified personal trainer to learn proper technique — this significantly reduces injury risk.
Walking is excellent for cardiovascular health, mental wellbeing, and calorie balance — and it is strongly encouraged for people on GLP-1 drugs. However, it does not provide a meaningful resistance stimulus for muscle preservation. Walking uses muscles, but it does not challenge them against enough resistance to trigger the muscle protein synthesis response that protects lean mass during caloric restriction. You need both: regular walking or cardio for heart health, plus dedicated resistance training at least twice a week for muscle preservation.
Yes. Standard clinical monitoring for GLP-1 therapy typically covers body weight, blood pressure, HbA1c or fasting glucose, and sometimes lipids. Body composition — the split between fat mass and lean mass — is rarely measured routinely, even though it is arguably more meaningful than scale weight alone. You can ask your prescriber about DXA body composition scanning at baseline and every 3–6 months during treatment. You can also self-monitor using a home bioimpedance scale, mid-arm muscle circumference measurements, and functional tests like timed stair climbing or grip strength. Being an informed, proactive patient on this topic leads to meaningfully better outcomes.
The most evidence-supported approach to muscle preservation is dietary protein — not supplements. That said, creatine monohydrate has a robust evidence base for supporting muscle mass and strength in adults, including older adults, and is generally considered safe. Vitamin D deficiency is common and is linked to reduced muscle function — having your levels checked and supplementing if deficient is sensible. Some researchers have explored whether medium-chain triglycerides such as C10 may help support muscle metabolism through nitrogen-sparing and anabolic signaling pathways, but this area is still being studied and no supplement should replace the foundational strategies of protein and resistance training. Always discuss any supplement with your healthcare provider before starting.
-
1
Wilding JPH, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine. 2021;384(11):989–1002. doi.org/10.1056/NEJMoa2032183
-
2
Look M, et al. "Body composition changes during weight reduction with tirzepatide in the SURMOUNT-1 study." Diabetes, Obesity and Metabolism. 2025;27(5):2720–2729. doi.org/10.1111/dom.16275
-
3
Neeland IJ, Linge J, Birkenfeld AL. "Changes in lean body mass with glucagon-like peptide-1-based therapies and mitigation strategies." Diabetes, Obesity and Metabolism. 2024;26(Suppl 4):16–27. doi.org/10.1111/dom.15728
-
4
Tinsley GM, Nadolsky S. "Preservation of lean soft tissue during weight loss induced by GLP-1 and GLP-1/GIP receptor agonists: A case series." SAGE Open Medical Case Reports. 2025. PMC12536186
-
5
Linge J, Birkenfeld AL, Neeland IJ. "Muscle mass and glucagon-like peptide-1 receptor agonists: adaptive or maladaptive response to weight loss?" Circulation. 2024. doi.org/10.1161/CIRCULATIONAHA.124.067676
-
6
Deer RR, Volpi E. "Protein intake and muscle function in older adults." Current Opinion in Clinical Nutrition & Metabolic Care. 2015;18(3):248–253. doi.org/10.1097/MCO.0000000000000162
-
7
Wilding JPH, et al. "Weight regain and cardiometabolic effects after withdrawal of semaglutide." Diabetes, Obesity and Metabolism. 2022;24(8):1553–1564. doi.org/10.1002/dom.14725
